
Page 15 - Volume13_Issue3
P. 15
VOLUME 13 | ISSUE 3
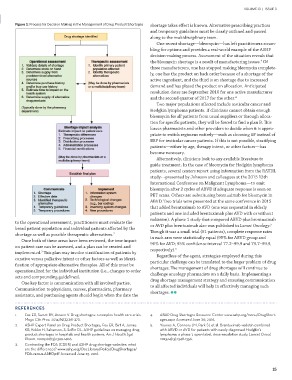
Figure 1: Process for Decision Making in the Management of Drug Product Shortages shortage takes effect is known. Alternative prescribing practices
and temporary guidelines must be clearly outlined and passed
to the operational assessment, practitioners must evaluate the along to the multidisciplinary team.
broad patient population and individual patients affected by the
shortage as well as possible therapeutic alternatives.2 One recent shortage—bleomycin—has left practitioners scram-
bling for options and provides a real-world example of the ASHP
Once both of these areas have been reviewed, the true impact decision-making process. Assessment of the situation reveals that
on patient care can be assessed, and a plan can be created and the bleomycin shortage is a result of manufacturing issues.4 Of
implemented.2 This plan may involve stratification of patients by three manufacturers, one has stopped making bleomycin complete-
curative versus palliative intent or other factors as well as identi- ly, one has the product on back order because of a shortage of the
fication of appropriate alternative therapies. All of this must be active ingredient, and the third is on shortage due to increased
operationalized for the individual institution (i.e., changes to order demand and has placed the product on allocation. Anticipated
sets and compounding guidelines). resolution dates are September 2016 for one active manufacturer
and the second quarter of 2017 for the other.4
One key factor is communication with all involved parties.
Communication to physicians, nurses, pharmacists, pharmacy Two major populations affected include testicular cancer and
assistants, and purchasing agents should begin when the date the Hodgkin lymphoma patients. If clinicians cannot obtain enough
bleomycin for all patients from usual suppliers or through alloca-
tion for specific patients, they will be forced to find a plan B. This
leaves pharmacists and other providers to decide when it is appro-
priate to switch regimens entirely—such as choosing EP instead of
BEP for testicular cancer patients. If this is not possible, stratifying
patients—either by age, therapy intent, or other factors—has
become necessary.
Alternatively, clinicians look to any available literature to
guide treatment. In the case of bleomycin for Hodgkin lymphoma
patients, several centers report using information from the RATHL
study—presented by Johnson and colleagues at the 2015 13th
International Conference on Malignant Lymphoma—to omit
bleomycin after 2 cycles of ABVD if adequate response is seen on
PET scans. Others are substituting brentuximab for bleomycin in
ABVD. Two trials were presented at the same conference in 2015
that added brentuximab to AVD (one was sequential in elderly
patients and one included brentuximab plus AVD with or without
radiation). A phase 1 study that compared ABVD plus brentuximab
or AVD plus brentuximab also was published in Lancet Oncology.5
Though it was a small trial (51 patients), complete response rates
in each arm were statistically equal (95% for ABVD group and
96% for AVD; 95% confidence interval 77.2–99.9 and 79.7–99.9,
respectively).5
Regardless of the agent, strategies employed during this
particular challenge can be translated to the larger problem of drug
shortages. The management of drug shortages will continue to
challenge oncology pharmacists on a daily basis. Implementing a
drug shortage management strategy and ensuring communication
to all affected individuals will help in effectively managing such
shortages.
REFERENCES 4. ASHP Drug Shortages Resource Center www.ashp.org/menu/DrugShort-
ages.aspx Accessed June 30, 2016.
1. Fox ER, Sweet BV, Jensen V. Drug shortages: a complex health care crisis.
Mayo Clin Proc. 2014;89(3):361-373. 5. Younes A, Connors JM, Park SI, et al. Brentuximab vedotin combined
with ABVD or AVD for patients with newly diagnosed Hodgkin’s
2. ASHP Expert Panel on Drug Product Shortages, Fox ER, Birt A, James lymphoma: a phase 1, open-label, dose-escalation study. Lancet Oncol.
KB, Kokko H, Salverson, S, Soflin DL. ASHP guidelines on managing drug 2013;14(13):1348-1356.
product shortages in hospitals and health systems. Am J Health Syst
Pharm. 2009;66(15):1399-1406.
3. Contrasting the FDA (CDER) and ASHP drug shortage websites: what
are the differences? www.ashp.org/DocLibrary/Policy/DrugShortages/
FDA-versus-ASHP.pdf Accessed June 25, 2016.
15